

The prevailing narrative that "schizophrenia ages you faster" has long shaped public and scientific understanding of this complex mental health condition. However, a landmark 2026 review by Fernandez-Egea, Garcia-Rizo, and Kirkpatrick, synthesizing findings from 170 studies across mortality, brain imaging, telomeres, epigenetic clocks, and metabolic markers, significantly reframes this assertion. While the signal of premature biological aging in individuals with schizophrenia is undeniable, the review argues that the term "accelerated" often overstates the dynamic for most biological systems measured after the illness’s onset. Instead, a more nuanced understanding suggests an "advanced" aging phenotype, where individuals start with a biological age deficit, maintaining a largely parallel decline to the general population, rather than experiencing a continuously steeper rate of aging. Crucially, the review also posits a more profound, and perhaps unsettling, possibility: that both the psychiatric illness and the observable aging phenotype may stem from shared upstream developmental damage, making the traditional "cause-and-effect" question far more intricate than previously conceived.
The Genesis of the "Accelerated Aging" Hypothesis
The concept of "schizophrenia as a syndrome of accelerated aging" was first formally articulated in a pivotal 2008 paper by Kirkpatrick and colleagues. This hypothesis emerged from a series of stark and perplexing observations that challenged the notion of schizophrenia as solely a brain disorder. Researchers noted that individuals diagnosed with schizophrenia face a significantly reduced life expectancy, dying, on average, 15 to 20 years earlier than the general population. Beyond premature mortality, they exhibited higher rates of dementia and developed metabolic diseases—such as type 2 diabetes and cardiovascular conditions—in their 20s and 30s, decades earlier than typically observed. If the condition were purely neurological, the rapid deterioration across multiple bodily systems seemed anomalous.
The original hypothesis posited schizophrenia as a multi-system condition where biological aging outpaces chronological aging across various organs and physiological markers. This framework predicted several key biological deviations: telomeres, the protective caps on chromosomes, should be shorter; inflammatory and oxidative-stress markers, indicators of cellular damage, should be elevated; brain volume and cognitive function should resemble those of older individuals; and mortality from age-linked diseases should occur earlier in life. The term "accelerated" carried a specific implication: a steeper slope of decline. This meant that if aging were truly accelerated in schizophrenia, the gap between patients and matched healthy controls would progressively widen over time, with patients losing biological ground faster year after year. It was this precise prediction that the 2026 review rigorously tested against 15 years of accumulated, multi-faceted data.
Mortality and Dementia Risk: Unambiguous Evidence
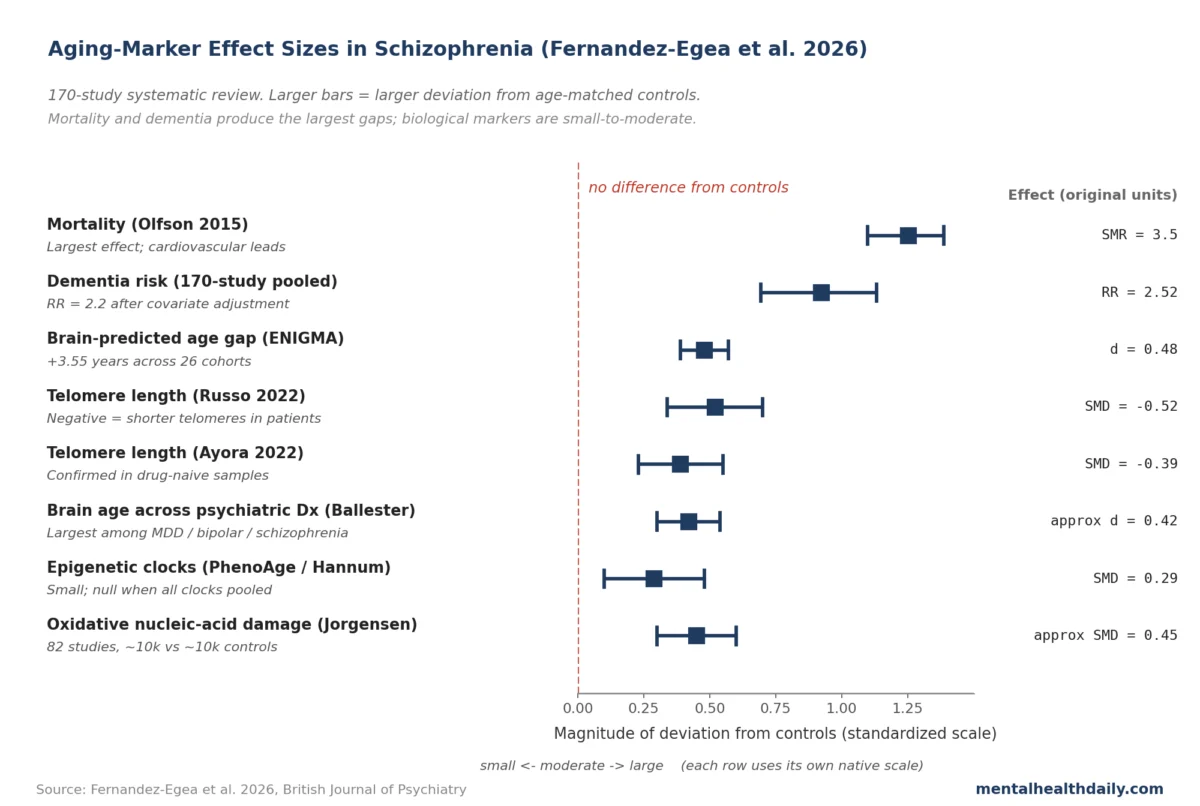
Among the numerous markers of biological aging, two areas consistently and strongly support the initial hypothesis of a profound impact: mortality and dementia risk. Individuals with schizophrenia face a standardized mortality ratio (SMR) typically ranging from 2.5 to 3.5 times that of the general population. This means they are 2.5 to 3.5 times more likely to die at any given age. Cardiovascular disease stands as the leading cause of this premature mortality, followed by suicide and accidental deaths. This mortality gap is not confined to specific healthcare systems or geographical regions, demonstrating its pervasive and systemic nature. Moreover, the risk of developing dementia is elevated by approximately 2.2 to 2.5 times, even after accounting for common cardiovascular risk factors. What is particularly striking is that dementia onset in this population typically occurs roughly two decades earlier than in the general population.
These two critical findings—premature mortality and heightened, earlier dementia risk—are robust, surviving stringent covariate adjustments for lifestyle factors and comorbidities. Crucially, they are also detectable in first-episode patients, often even before chronic exposure to antipsychotic medications, firmly establishing them as intrinsic aspects of the illness trajectory rather than mere consequences of treatment. These facts form the strongest pillars upholding the framing of schizophrenia as a disorder intrinsically linked to altered aging processes.
Biological Markers: A Closer Look at Brain Age, Telomeres, and Epigenetic Clocks
Beyond broad epidemiological observations, the 2026 review delved into specific biological markers that offer more granular insights into cellular and systemic aging. Three markers—brain age, telomere length, and epigenetic clocks—have accumulated the most extensive data, revealing consistent deviations, though often smaller and more complex than popular understanding suggests.
Brain Age: Neuroimaging studies employing machine learning algorithms to estimate "brain age" consistently report that individuals with schizophrenia exhibit brains that appear biologically older than their chronological age. A comprehensive ENIGMA meta-analysis, encompassing 26 cohorts, estimated an average brain age elevation of approximately 3.5 years (95% CI 2.91–4.19). This "older" brain appearance is characterized by differences in structural MRI features such as reduced grey matter volume, altered white matter integrity, and larger ventricular volumes. Importantly, this brain-age gap is already evident at the time of the first psychotic episode, with reported deviations ranging from +1.4 to +6.9 years across various studies. Longitudinal data generally indicate that this gap tends to hold steady over follow-up periods of 5-10 years, suggesting a level-shift rather than a continuously accelerating decline in brain structure after illness onset. However, it’s worth noting that these deviations are also measurable in individuals classified as clinical-high-risk (CHR) for psychosis, even before they receive a formal diagnosis, hinting at pre-diagnostic biological changes.
Telomere Length: Telomeres, the protective DNA-protein complexes at the ends of chromosomes, shorten with each cell division and are considered a key biomarker of cellular aging and overall health. Multiple meta-analyses (e.g., SMD around -0.39 to -0.52) have consistently shown that individuals with schizophrenia have shorter telomeres compared to healthy controls. This shortening is not a trivial finding; it reflects accelerated cellular senescence and is associated with increased risk for various age-related diseases. Similar to brain age, shorter telomere lengths have been observed in drug-naive, first-episode patients, indicating that this biological deviation predates chronic pharmacological intervention. The evidence also suggests that telomere shortening appears early in the illness course and does not necessarily worsen significantly over time, again aligning with an "advanced" rather than uniformly "accelerated" pattern.
Epigenetic Clocks: These biochemical tests estimate biological age by measuring methylation patterns on DNA. Different epigenetic clocks (e.g., Horvath, Hannum, GrimAge) are designed to capture various aspects of aging, from intrinsic cellular aging to mortality risk and cumulative damage. The "epigenetic story" in schizophrenia is, by far, the most complex and "messiest" of the three markers. While some clocks might indicate a degree of acceleration, others show contradictory results, or even a deceleration in certain youth-stage contexts. The pooled effects across all epigenetic clocks in schizophrenia are often small and highly dependent on the specific clock used, making a uniform "accelerated aging" verdict difficult to establish. This inconsistency underscores a critical challenge in the field: understanding precisely what each epigenetic clock measures and how applicable it is to pathological conditions like schizophrenia, which involve unique biological stressors. The disagreement among clocks is a primary reason why the "accelerated" framing breaks down most clearly in this domain.
The pooled effect sizes across these major aging markers, as summarized in the original article’s accompanying chart, clearly illustrate this hierarchy: mortality and dementia risk show large effect sizes, brain age and telomere markers exhibit moderate effects, while epigenetic clock effects are generally small and highly variable.
Advanced vs. Accelerated: A Critical Distinction
The 2026 review’s central re-reading hinges on a crucial distinction often overlooked in popular discourse: the difference between a "level-shift" and a "steeper slope" in biological aging trajectories.
- Level-shift (Advanced Aging): In this model, biological-age markers in individuals with schizophrenia are already deviated from healthy controls at the time of the first episode. From that point onward, the rate of biological decline tracks largely parallel to that of healthy aging. The trajectory lines run offset, but at a similar gradient, meaning the gap between patients and controls remains relatively constant over time.
- Steeper Slope (Accelerated Aging): This model implies that the gap between patients and controls progressively widens over time. Individuals with schizophrenia would lose biological ground at a faster rate than healthy controls, year after year.
Longitudinal data for most markers, particularly global neuroimaging and cognitive trajectories after illness onset, predominantly favor the level-shift reading. Brain-age studies, for instance, consistently find first-episode patients already exhibiting brains that appear 1.4 to 6.9 years "older" than their chronological age. Critically, this initial gap tends to remain stable over 5 to 10 years of follow-up. Similarly, cognitive studies show first-episode patients performing at a level comparable to healthy adults 5 to 10 years their senior, with performance largely tracking stably thereafter, except for a subset (approximately 10% in some studies) who experience a later decline often tied to negative symptoms. Telomere shortening also appears early and does not show a clear pattern of worsening over time.
However, this "advanced, not accelerated" verdict comes with an important methodological caveat. The parallel-trajectory finding is based on measurements initiated at the first episode. If significant biological accumulation or accelerated decline were occurring during the prodromal period—the typically 2-5 year phase preceding a formal diagnosis—the observed pattern at illness onset would still appear as a static level-shift. In other words, a gap present at onset that then tracks parallel afterward could mask earlier acceleration. The review’s own data lends credence to this possibility: studies of clinical-high-risk individuals who have not yet received a formal diagnosis already show brain-age deviations of +1.4 to +6.9 years. A static biological shift appearing only at illness onset would logically not be detectable before onset. This strongly suggests that biological changes are accumulating even before the full-blown psychotic episode.
The authors are also careful to acknowledge that the level-shift model may not apply uniformly across all biological systems. They explicitly note that "true acceleration seems to be less common and may be confined to specific systems," citing rapid brain volume loss in the first 5 years of illness and cumulative oxidative stress accumulation over chronicity as potential exceptions. Thus, while the "advanced not accelerated" verdict applies most cleanly to global neuroimaging and cognitive trajectories post-onset, it doesn’t negate the possibility of accelerated decline in specific, critical domains.
Early Developmental Scars: A Neurodevelopmental Reframe
Perhaps the most significant conceptual contribution of the 2026 review, which goes beyond the terminology debate, is the causal model proposed in its discussion section. This model suggests a profound paradigm shift in understanding the relationship between schizophrenia and biological aging. The authors argue that the aging phenotype observed in schizophrenia and the psychiatric diagnosis itself may both be downstream consequences of the same early developmental insults, rather than schizophrenia directly causing the aging. This reframes the entire causal question.
Three compelling lines of evidence support this neurodevelopmental framing:
- Shared Risk Factors: Widely replicated risk factors for schizophrenia, such as prenatal stress (e.g., maternal infection, severe nutritional deficiencies), childhood adversity (e.g., trauma, abuse, neglect), and early inflammatory insults, are also independently established drivers of various biological aging markers. For example, early life stress is known to shorten telomeres, disrupt metabolic regulation, and alter epigenetic profiles, contributing to premature aging.
- Genetic Overlap: There is a notable overlap between polygenic risk variants for schizophrenia and genetic pathways associated with inflammation, oxidative stress, and metabolic dysregulation, all of which are fundamental to the process of biological aging. This shared genetic architecture suggests a common underlying vulnerability that manifests as both psychiatric illness and an accelerated aging trajectory.
- Pre-Diagnosis Deviations: As previously mentioned, biological aging markers, such as brain-age deviations, are already present in clinical-high-risk individuals even before they receive a formal diagnosis of schizophrenia. This indicates that the biological underpinnings of accelerated aging are not merely a consequence of established illness or its treatment, but rather emerge earlier in the developmental trajectory, potentially alongside the prodromal phase of the disorder.
The authors eloquently describe the multisystem aging observed in schizophrenia as "the long-term trajectory of early developmental scars." These early insults, occurring during critical periods of neurodevelopment, not only confer an increased vulnerability to psychiatric illness but also predispose individuals to progressive degeneration, both physical and mental, throughout their lifespan.
The practical implications of this neurodevelopmental reframing are profound. It suggests that simply asking whether schizophrenia "causes" accelerated aging may be a partially misframed question. Instead, both the psychiatric illness and the biological aging phenotype may be parallel expressions of the same upstream developmental exposures. Consequently, the most impactful interventions would not solely focus on managing aging consequences after illness onset, but rather on targeting the earliest possible developmental vulnerabilities. This includes addressing prenatal stress, mitigating childhood adversity, and managing early inflammatory burdens, thereby potentially addressing both the psychiatric and somatic risks simultaneously before they become entrenched.
The Role of Antipsychotic Medications
A frequently asked and often contentious question is whether antipsychotic medications themselves contribute to or cause the observed aging phenotype in schizophrenia. The evidence addresses two distinct aspects: whether antipsychotics are the origin of the aging phenotype, and whether they worsen or accelerate it once present.
Regarding the origin, the evidence is clear: antipsychotics are not the primary cause. Several key aging signals, including impaired glucose regulation, elevated inflammatory cell counts, lower free testosterone levels, shortened telomere length, and brain-age elevations, are demonstrably present in antipsychotic-naive first-episode patients. This robust finding confirms that the biological deviation predates chronic medication exposure.
However, this does not fully exonerate antipsychotics on the second question: whether they worsen or amplify the existing aging trajectory. While not the origin, antipsychotics can undeniably exacerbate specific aspects of the aging phenotype. Second-generation antipsychotics, such as olanzapine and clozapine, are well-known to induce significant weight gain, insulin resistance, and dyslipidemia in a substantial proportion of users. These metabolic side effects contribute directly to the heightened risk of cardiovascular disease, a leading cause of premature mortality in schizophrenia. Furthermore, cumulative anticholinergic exposure, stemming from certain antipsychotics and adjunctive medications, is increasingly recognized as a significant driver of early cognitive decline, which initially contributed to the "accelerated aging" framing. The review concedes that antipsychotics "amplify specific subdomains" without definitively quantifying the magnitude of this amplification over decades of treatment.
The consensus from the scientific community is that discontinuing antipsychotics is generally not the solution. These medications are crucial for managing psychotic symptoms, preventing relapse, and significantly reducing the risk of suicide and accidental deaths, benefits that typically outweigh their metabolic costs for most patients. Instead, the focus for clinicians and patients is on proactive prevention and management: rigorous metabolic monitoring, comprehensive lifestyle support (diet, exercise), and minimizing anticholinergic burden where clinically feasible by careful medication selection and dose adjustment.
Unresolved Questions and Gaps in the Literature
Despite the significant advancements offered by the 2026 review, several critical gaps and methodological challenges persist in the schizophrenia aging literature:
- The "Baseline Problem" for Advanced vs. Accelerated: The "advanced not accelerated" conclusion relies on evidence starting at first episode. As discussed, if significant biological accumulation occurs during the prodromal phase (2-5 years before diagnosis), it would present as an immediate "level-shift" at onset. The review acknowledges this indirectly through clinical-high-risk data but does not fully resolve the question of whether true acceleration occurs before diagnosis.
- Unresolved Genetic Confounding: Schizophrenia’s polygenic risk variants overlap with pathways implicated in inflammation, oxidative stress, and metabolic regulation—all independent drivers of biological aging. It remains challenging to disentangle whether "schizophrenia caused this" from "a shared genetic architecture caused both." While Mendelian randomization designs offer a powerful tool to probe causal direction by using genetic variants as natural experiments, they have yielded mixed findings across various biomarkers, indicating the complexity of the genetic interplay.
- Survival Bias in Older Cohorts: Studies focusing on older adults (e.g., 60+) with schizophrenia are inherently subject to survival bias. The individuals who live long enough to be studied in these age groups often represent a healthier, more resilient subset, as the most vulnerable individuals with the most severe aging phenotypes may have already succumbed to illness-related complications. This bias can artificially flatten apparent aging trajectories in older samples, underestimating the true impact.
- Antipsychotic Confounding in Chronic Samples: The vast majority of chronic-stage data in schizophrenia comes from medicated patients. Drug-naive samples are typically smaller and followed for shorter durations. This makes it exceedingly difficult to cleanly disentangle the natural progression of aging in schizophrenia from the long-term effects of medication. Therefore, what is often described as the "natural history of schizophrenia aging" is, in reality, largely the "treated schizophrenia aging."
- Biomarkers Calibrated on Healthy Populations: Many widely used aging biomarkers, such as brain-age algorithms and epigenetic clocks, were initially developed and calibrated using cohorts of healthy individuals without major psychiatric illness. When applied to a population with schizophrenia, these measures may pick up a broader "cumulative biological burden" related to the illness, its treatments, lifestyle factors, and comorbidities, rather than purely reflecting an acceleration of the intrinsic aging process per se. The review explicitly acknowledges that these measures "may reflect cumulative biological burden rather than ageing per se."
- Smoking as a Major Confounder: Smoking rates among individuals with schizophrenia are alarmingly high, often ranging from 60-80%, significantly higher than the general population. This lifestyle factor is a potent driver of premature aging. Studies have shown that a substantial portion of the observed "aging effect," particularly for specific epigenetic clocks like GrimAge and several inflammatory markers, significantly diminishes or even disappears after rigorous adjustment for smoking status. This highlights that a significant component of the "aging effect" is, in fact, a "smoking effect."
- Disagreement Among Epigenetic Clocks: The lack of consistent findings across different epigenetic clocks in schizophrenia is a major challenge. Different clocks are trained on different sets of CpG sites and designed to predict different outcomes (e.g., chronological age, mortality, healthspan). Until the field achieves a better understanding of what each specific clock truly measures and its relevance in a complex illness like schizophrenia, interpreting pooled effects or drawing definitive conclusions about epigenetic aging remains difficult.
Implications for Prevention and Intervention: A Call for Upstream Approaches
The evolving understanding of schizophrenia and biological aging carries profound implications for clinical practice and public health. If the deviation in biological age largely arrives at or even before the formal onset of illness, the interventions with the highest leverage must occur at or near the first contact with mental health services, rather than years into chronic illness. This underscores the critical importance of early intervention programs that address not just psychiatric symptoms but also physical health risks from the outset.
Furthermore, if the neurodevelopmental framing is accurate—that early developmental insults represent the deeper causal structure underlying both the psychiatric illness and the aging phenotype—then the most impactful leverage point lies even earlier. Interventions targeting these fundamental exposures, such as comprehensive prenatal care, strategies to mitigate childhood adversity and trauma, and approaches to manage early inflammatory burdens, hold the potential to address both the psychiatric and somatic risks before either becomes established. This calls for a truly integrated, lifespan approach to care, extending from preconception and early childhood through adulthood.
Practical recommendations stemming from this research include:
- Smoking Cessation Programs: Aggressive and sustained efforts to support smoking cessation are paramount, given its substantial contribution to premature aging and overall poor health outcomes.
- Metabolic Monitoring and Management: Routine and thorough screening for metabolic abnormalities (e.g., weight, blood pressure, lipids, glucose) must be standard practice, coupled with proactive interventions for early detection and management.
- Lifestyle Support: Comprehensive lifestyle interventions encompassing diet, regular physical exercise, and stress reduction techniques are essential to mitigate cardiovascular risk and promote overall well-being.
- Pharmacological Optimization: Clinicians should strive to minimize anticholinergic burden where clinically appropriate and consider lower-metabolic-risk antipsychotics when effective and tolerable for the patient.
In conclusion, the narrative around schizophrenia and aging is shifting from a simplistic "accelerated aging" to a more nuanced understanding of "advanced aging," characterized by an early biological age deficit that largely tracks parallel to healthy aging post-onset. This shift is accompanied by a powerful neurodevelopmental reframe, suggesting that both the illness and the aging phenotype may be manifestations of shared early developmental scars. This evolving perspective does not diminish the gravity of premature aging in schizophrenia but redirects our focus toward more targeted, earlier, and more holistic interventions, ultimately aiming to improve both the mental and physical health trajectories for individuals living with this challenging condition.
