

A groundbreaking examination of surgical interventions, particularly those aimed at weight loss and orthopedic issues, has brought to light a disquieting truth: some of the most widely performed and promoted procedures may offer little to no tangible benefit beyond a placebo effect. Investigations, including meticulously designed sham surgery trials, suggest that the perceived efficacy of certain popular surgeries is significantly inflated, raising critical questions about patient care, medical industry practices, and the very definition of evidence-based medicine.
The Rise and Fall (and Resurgence) of the Gastric Balloon
The intragastric balloon, a device introduced in the 1980s with considerable fanfare, promised a less invasive approach to weight management. The concept was straightforward: implanting a balloon into the stomach and inflating it with air or water to create a feeling of fullness, thereby reducing food intake. This innovation arrived amidst a growing awareness of the obesity epidemic and a demand for novel solutions. However, as is often the case with medical devices, the intragastric balloon was brought to market with insufficient robust evidence of its long-term effectiveness and safety.
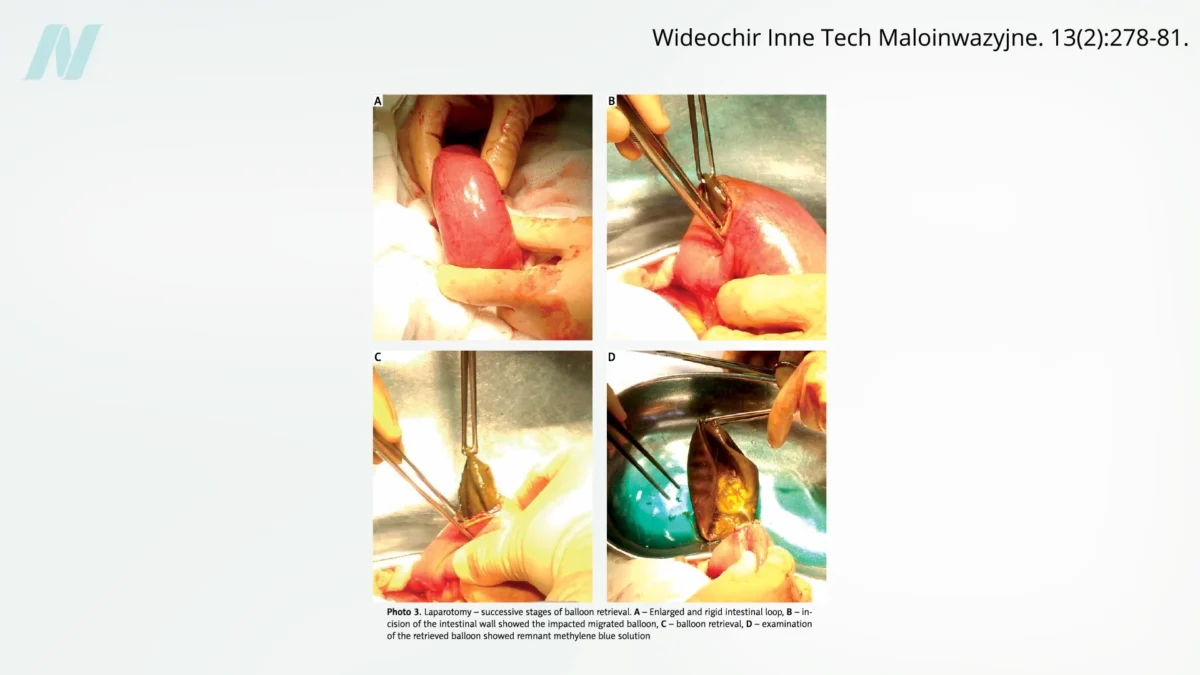
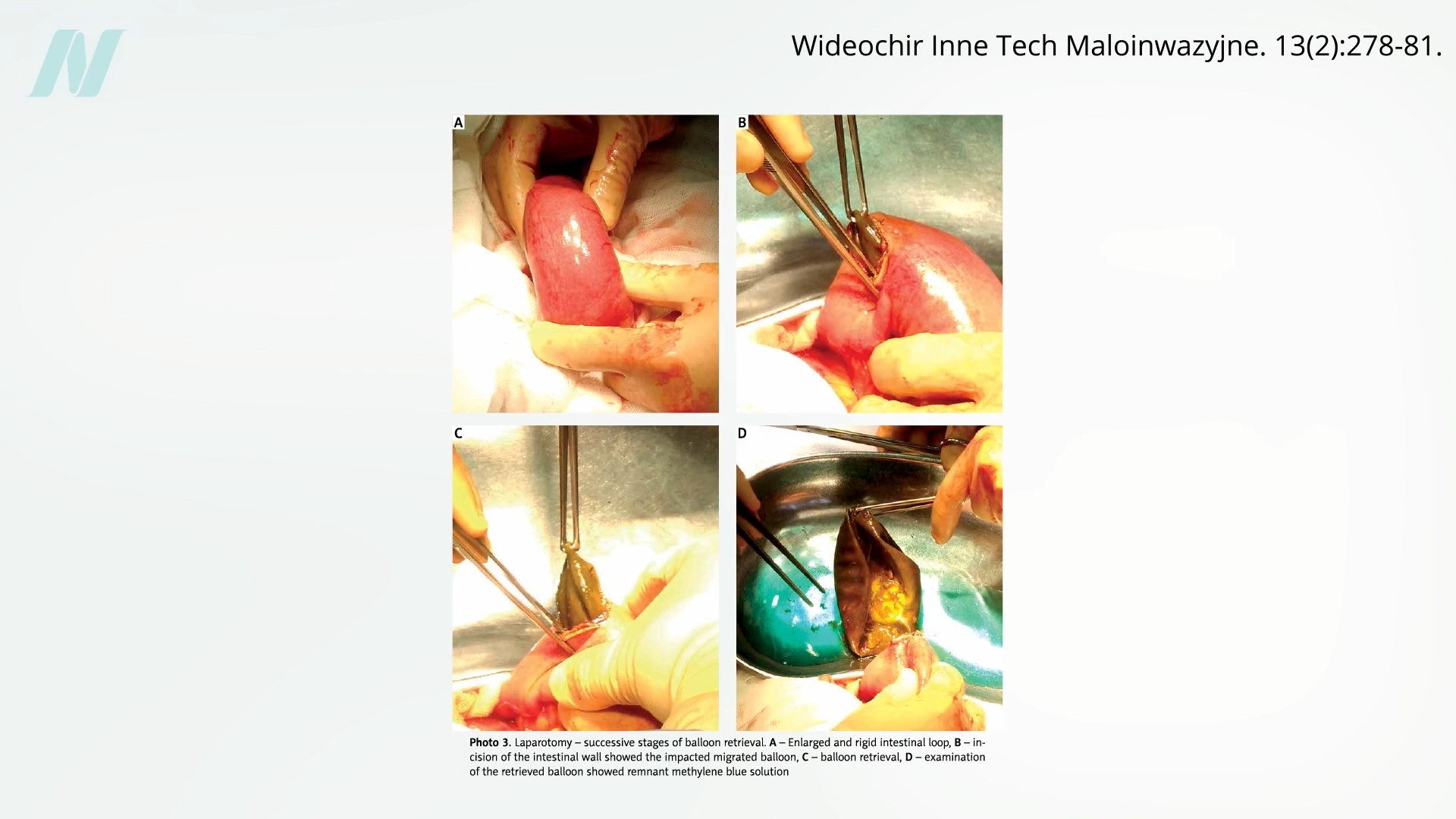
Early clinical experiences soon revealed significant shortcomings. A pivotal study conducted at the Mayo Clinic, published in the early 1990s, delivered a stark assessment: a staggering 80% of intragastric balloons spontaneously deflated. This malfunction presented a serious risk, as a deflated balloon could migrate into the intestines, leading to potentially life-threatening bowel obstruction. The visual evidence, including radiological imaging, starkly illustrated this hazard, with deflated balloons creating blockages in the intestinal tract.
Beyond the risk of mechanical failure, the balloons also proved to be physiologically problematic even before deflation. Data indicated that approximately half of the patients experienced gastric erosions, a condition involving damage to the stomach lining. This mucosal damage could lead to pain, bleeding, and other gastrointestinal disturbances.
Perhaps the most damning finding, however, was the lack of demonstrable superiority over conservative weight-loss methods. When compared to structured diet plans and behavioral modification strategies, the intragastric balloon failed to deliver significantly better or more sustainable weight loss outcomes. Consequently, the initial wave of intragastric balloons was ultimately withdrawn from the market due to these safety concerns and questionable efficacy.

The Return of the Balloon and Industry Influence
Despite its troubled past, the intragastric balloon made a significant comeback. In 2015, the U.S. Food and Drug Administration (FDA) began approving a new generation of these devices. This resurgence coincided with the passage of the Sunshine Act, legislation designed to increase transparency in financial relationships between healthcare providers and the pharmaceutical and medical device industries. The act mandates the disclosure of payments made by these companies to physicians, aiming to shed light on potential conflicts of interest.
While the Sunshine Act has brought greater awareness to the financial ties between doctors and "Big Pharma," the influence of device manufacturers on surgeons is a less publicized, yet equally potent, factor. Reports have surfaced detailing substantial payments from medical device companies to physicians, with the top 100 recipients accumulating an astonishing $12 million from these entities in a single year. Disturbingly, a significant minority of physicians receiving these payments failed to disclose these conflicts of interest when publishing research related to the devices they used, underscoring a persistent challenge in maintaining objective scientific reporting.
The modern intragastric balloons, while still carrying risks, are often marketed with the advantage of being reversible, unlike many more invasive bariatric surgical procedures. However, reversibility does not equate to benignity. The FDA has issued a series of advisories highlighting serious risks associated with these devices, including the potential for death.
One of the more unexpected and severe complications is gastric perforation. This can occur not through direct trauma from the smooth, rounded balloon itself, but indirectly. The balloons frequently induce severe nausea and vomiting, which are reported as very common side effects, affecting a majority of recipients. Persistent and forceful vomiting can, in extreme cases, lead to a rupture of the stomach wall, a catastrophic event with a high mortality rate. These episodes of intense vomiting are also believed to contribute to life-threatening nutrient deficiencies, a concerning consequence for individuals seeking to improve their health through weight loss.
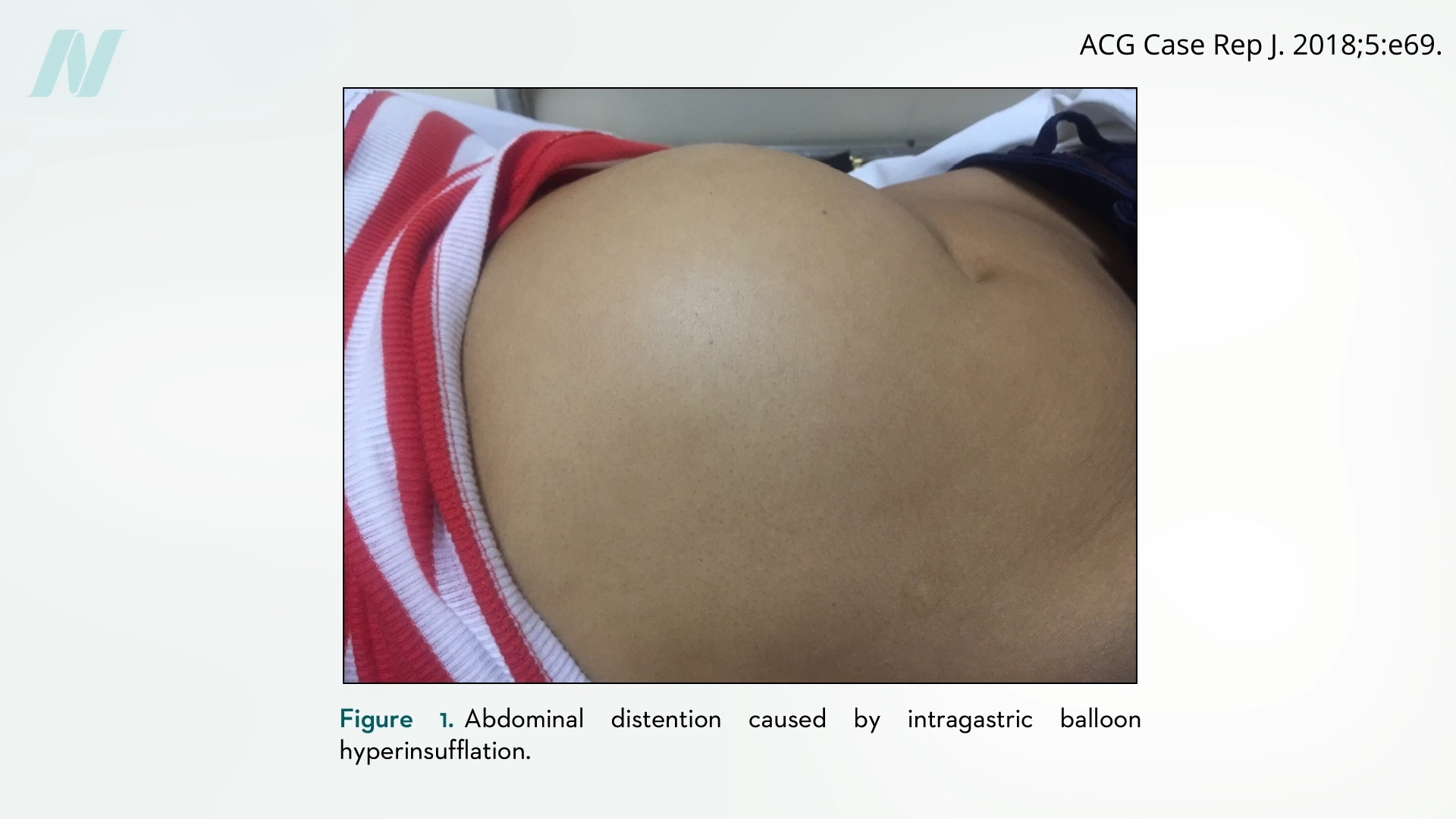
Complications can arise from both under- and over-inflation. While deflated balloons can lead to bowel obstructions, some devices have been observed to suddenly overinflate. This phenomenon, mirroring issues previously seen with breast implants, can cause severe abdominal pain, vomiting, and distention, presenting acute medical emergencies. The "spontaneously autoinflating" nature of some medical devices, as documented in the context of breast implants, remains a poorly understood and underreported concern within the medical community. Notably, early experimental intragastric balloons were, in some instances, derived from modified breast implant technology, highlighting a continuum of device-related challenges.
The Uproar of Sham Knee Surgery Trials
The concept of "sham surgery" as a control in clinical trials emerged as a response to the inherent difficulties in isolating the true therapeutic effect of surgical interventions. Unlike pharmaceutical trials where inert placebos (sugar pills) can be used, blinding patients and surgeons to the actual performance of a procedure is far more complex. The placebo effect in surgery, driven by patient expectation, surgeon attention, and the procedural experience itself, can be substantial, making it difficult to ascertain whether observed improvements are due to the intervention or the context of care.
In 2002, a landmark study published in The New England Journal of Medicine applied the sham surgery methodology to one of the most frequently performed orthopedic procedures: arthroscopic surgery of the knee. Billions of dollars are expended annually on arthroscopic interventions for osteoarthritis and knee injuries, involving the insertion of small cameras (arthroscopes) and surgical instruments into the knee joint to debride or repair damaged tissue.
The trial, led by researchers at the Medical University of South Carolina, recruited patients suffering from chronic knee pain. These participants were randomly assigned to one of three groups: those who underwent the full arthroscopic procedure, those who received a partial procedure (involving only superficial incisions), and a sham surgery group. In the sham procedure, surgeons made incisions and simulated the steps of arthroscopic surgery, including irrigating the joint with saline, but did not actually perform any joint debridement or repair. This rigorous design was intended to control for the placebo effect and the surgical ritual itself.
The publication of these findings ignited a firestorm of controversy within the medical and professional communities. Medical associations and ethicists alike questioned the morality of subjecting patients to incisions and surgical procedures that were intentionally non-therapeutic. Concerns were raised about the potential psychological impact on patients who discovered they had undergone a "fake" surgery, and the ethical implications for the surgeons involved.
However, the results of the trial were undeniable and profoundly challenging to the established norms of orthopedic surgery. Both the patients who received the actual arthroscopic surgery and those who underwent the sham procedure reported significant improvements in their knee pain and function. Crucially, there was no statistically significant difference in outcomes between the groups. This suggested that the perceived benefits of arthroscopic knee surgery for osteoarthritis and degenerative knee injuries were largely attributable to the placebo effect, rather than any specific therapeutic action of the procedure itself. The implication was that billions of dollars were being spent annually on a surgery that, for many patients, offered no superior benefit to a simulated intervention.
This revelation has had a ripple effect, prompting similar scrutiny of other widely practiced surgical procedures. Rotator cuff shoulder surgery, for instance, is currently facing a comparable crisis of confidence, with emerging research questioning its efficacy in certain patient populations when compared to non-operative treatments or sham interventions.
Re-evaluating Weight Loss Devices and Surgical Claims
The lessons learned from sham surgery trials are directly applicable to the evaluation of weight-loss interventions, including the intragastric balloon. When these devices are subjected to sham-controlled studies, the results are often sobering. These investigations have revealed that many older and newer intragastric balloon models fail to provide any significant, lasting weight loss benefit.
Even in instances where some weight loss is observed, it is often temporary. Intragastric balloons are typically designed for short-term use, generally limited to six months. This duration is partly dictated by the increasing risk of deflation and associated complications beyond this timeframe. Attempts to extend the use of balloons or to replace them with new ones have not demonstrated improved long-term weight management outcomes in sham-controlled trials. Furthermore, the effects on appetite and satiety, key mechanisms by which balloons are thought to induce weight loss, appear to diminish over time, suggesting that the body may adapt to the presence of the device.
The Broader Implications: "Fake News" in Medicine
The consistent findings from sham surgery trials present a profound challenge to the medical profession. Doctors often pride themselves on their adherence to scientific principles and their opposition to pseudoscience, such as the anti-vaccination movement or the trend of individuals "choosing their own facts." However, the evidence from these surgical studies suggests that the medical field is not immune to its own brand of "fake news" and "alternative facts."
When popular surgical procedures are found to be ineffective, and in some cases, may even exacerbate existing conditions (such as increasing the risk of progression to a total knee replacement following non-therapeutic knee surgery), it raises serious ethical and practical questions. The financial incentives for device manufacturers and surgeons, coupled with the inherent power of the placebo effect, can create an environment where procedures are promoted and performed without adequate scientific justification.
The implications are far-reaching:
- Patient Trust: The revelation that popular surgeries may be ineffective erodes patient trust in the medical system. Patients undergo these procedures with the expectation of genuine therapeutic benefit and often incur significant costs, both financial and in terms of recovery time and potential complications.
- Healthcare Spending: Billions of dollars are spent annually on surgical interventions that may offer little to no real benefit. Reallocating these resources towards evidence-based, less invasive, or preventative health strategies could lead to more effective and efficient healthcare.
- Medical Education and Practice: There is a critical need for a re-evaluation of surgical training and continuing medical education. Emphasizing rigorous scientific methodology, critical appraisal of evidence, and transparency in industry relationships is paramount.
- Regulatory Oversight: Regulatory bodies like the FDA face ongoing challenges in ensuring that medical devices and surgical procedures are rigorously tested for safety and efficacy before widespread adoption. Post-market surveillance must be robust and responsive to emerging evidence.
The findings from sham surgery trials serve as a critical reminder that the practice of medicine must continually be grounded in rigorous scientific inquiry and a commitment to patient well-being above all else. As the medical community grapples with these unsettling truths, a renewed focus on evidence-based practice and ethical transparency is essential to ensure that patients receive the most effective and appropriate care.
Doctor’s Note: This article is part of a two-part series exploring the effectiveness of various weight-loss interventions. The subsequent installment, "Extreme Weight-Loss Devices," will delve into other technologies and their scientific validation. For further information on bariatric surgery and weight management, please refer to related posts and resources. My book, How Not to Diet, offers a comprehensive guide to sustainable weight loss strategies, available through libraries and booksellers. All proceeds from book sales are donated to charity.
