

The landscape of treating type 2 diabetes, particularly for individuals struggling with obesity, has long been shaped by the advancements and perceived efficacy of bariatric surgery. While surgical interventions have demonstrated significant success in achieving diabetes remission, emerging research and a closer examination of the underlying mechanisms suggest that the benefits may stem less from the anatomical alterations themselves and more from the profound caloric restriction that accompanies these procedures. This paradigm shift challenges the prevailing narrative and calls for a re-evaluation of treatment strategies, emphasizing the potent therapeutic potential of dietary interventions.
The Rise of "Metabolic Surgery" and Its Promise
For years, bariatric surgery has been recognized for its substantial impact on weight loss, often leading to remarkable improvements in obesity-related comorbidities, including type 2 diabetes. The surgical community, in an effort to reframe the procedure beyond its more aggressive descriptions, has adopted the term "metabolic surgery." This nomenclature aims to highlight the physiological changes that occur post-surgery, suggesting that the internal rearrangements of the gastrointestinal tract trigger beneficial hormonal shifts that contribute to metabolic health.
A cornerstone of this argument has been the impressive remission rates for type 2 diabetes observed in patients undergoing bariatric procedures. Studies have indicated that approximately 50% of obese individuals with type 2 diabetes, and a striking 75% of those classified as "super-obese" with the condition, experience remission. This remission is defined by the achievement of normal blood sugar levels without the need for diabetes medication, a state that can manifest within days of the surgery. Furthermore, long-term follow-up data has shown that around 30% of patients remain diabetes-free 15 years post-surgery, a figure that significantly outpaces the roughly 7% remission rate observed in non-surgical control groups.
Unpacking the Surgical Process and Its Precursors
However, the surgical process itself is not without its challenges and inherent risks. A critical and often demanding step in many bariatric procedures involves manipulating the liver. In obese individuals, the liver is frequently enlarged and laden with fat, increasing the risk of intraoperative injury and bleeding. This enlarged liver is a common reason why less invasive laparoscopic surgeries may need to be converted to more extensive open procedures, resulting in larger scars, increased risk of wound infections, and prolonged recovery times.

Recognizing these risks, and the fact that even a modest weight loss of 5% can lead to a significant reduction in liver fat (potentially by 10%), patients awaiting bariatric surgery are typically placed on a strict pre-operative diet. This dietary regimen, often involving extremely low-calorie liquid intake for several weeks both before and after surgery, has been a standard component of the bariatric patient pathway. This practice raises a crucial question: could the observed improvements in blood sugar levels and diabetes remission be primarily attributable to this intensive caloric restriction, rather than a unique "metabolic magic" derived from the surgical alterations?
A Groundbreaking Study: Isolating the Impact of Caloric Restriction
To address this critical question, researchers at the University of Texas embarked on a novel study designed to disentangle the effects of bariatric surgery from the impact of severe caloric restriction. Patients with type 2 diabetes who were scheduled for gastric bypass surgery volunteered to participate in a controlled experiment.
The study involved two phases for the same group of patients. In the first phase, participants remained hospitalized for 10 days and adhered to an extremely low-calorie diet (less than 500 calories per day), mirroring the pre- and post-operative dietary protocols, but without undergoing surgery. After a period of regaining the lost weight, these same patients then underwent the actual gastric bypass surgery. Following the surgery, they repeated the identical low-calorie diet, meticulously matched day-by-day to their initial dietary period. This innovative design allowed researchers to directly compare the physiological outcomes of caloric restriction with and without the surgical intervention, using the same individuals and the same dietary regimen. The hypothesis was that if anatomical rearrangement conferred a unique metabolic advantage, patients would show superior results after surgery.
Surprising Findings: Caloric Restriction Emerges as the Primary Driver
The results of this meticulously designed study were both surprising and illuminating. Contrary to the expectation that surgery would yield superior outcomes, the findings indicated that caloric restriction alone resulted in comparable, and in some measures, significantly better, improvements in blood sugar levels, pancreatic function, and insulin sensitivity. In several key indicators of diabetic control, patients actually performed better when the low-calorie diet was implemented without the surgical procedure. The surgery, in this context, appeared to place patients at a metabolic disadvantage.
The Physiology of Reversal: Fat Mobilization and Insulin Sensitivity
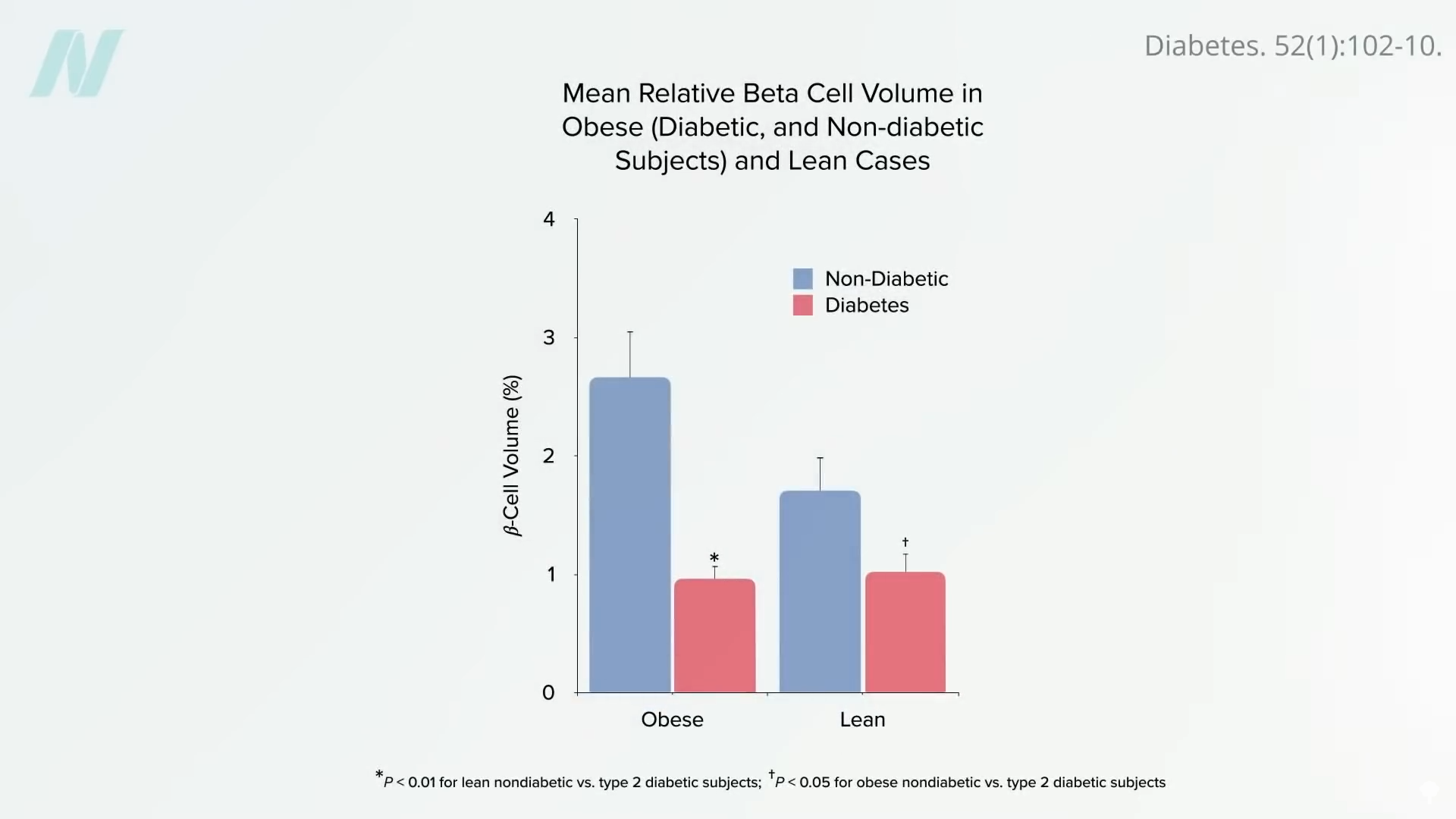
The underlying mechanism for these findings lies in the profound impact of caloric restriction on fat accumulation within the body, particularly in the liver and pancreas. Type 2 diabetes is increasingly understood as a condition driven by excess fat deposition in these vital organs. When an individual exceeds their "personal fat threshold," fat begins to accumulate in the liver, leading to insulin resistance. The liver may then attempt to offload this excess fat by releasing very-low-density lipoproteins (VLDL) into the bloodstream. This fat can subsequently accumulate in the pancreas, impairing the function of the insulin-producing beta cells. By the time type 2 diabetes is diagnosed, a substantial proportion of these essential cells may have already been destroyed.
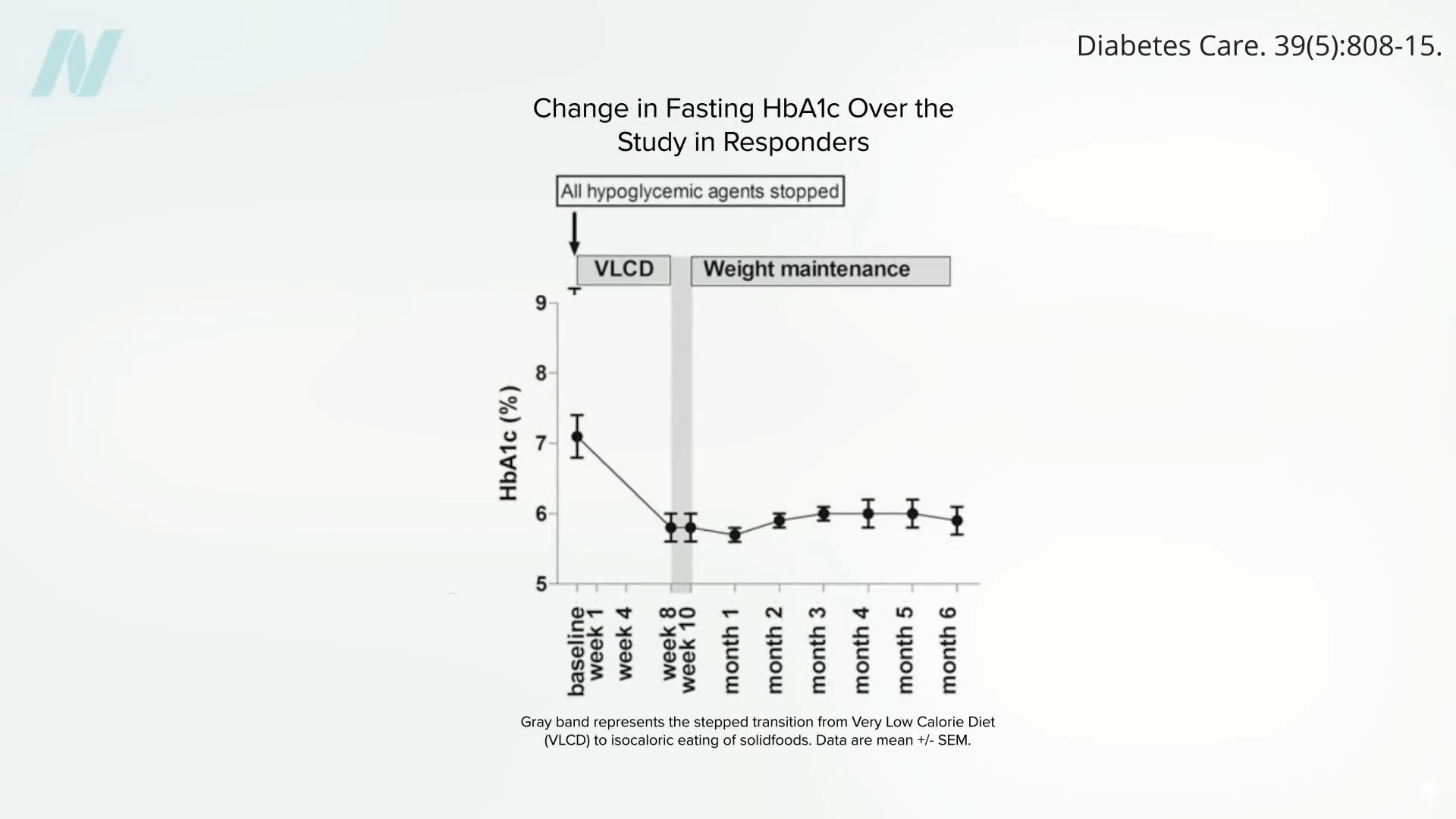
However, the study highlights that a significant caloric deficit can effectively reverse this process. Within as little as seven days of a substantial calorie reduction, liver fat can decrease dramatically, restoring hepatic insulin sensitivity. Sustaining this caloric deficit for approximately eight weeks can lead to a normalization of pancreatic fat levels and improved function. Crucially, once an individual drops below their personal fat threshold, they may be able to resume normal caloric intake without experiencing a recurrence of diabetes. This suggests that the body has a remarkable capacity for self-repair when provided with the right physiological conditions.
Weight Loss and Diabetes Remission: A Question of Quantity and Quality
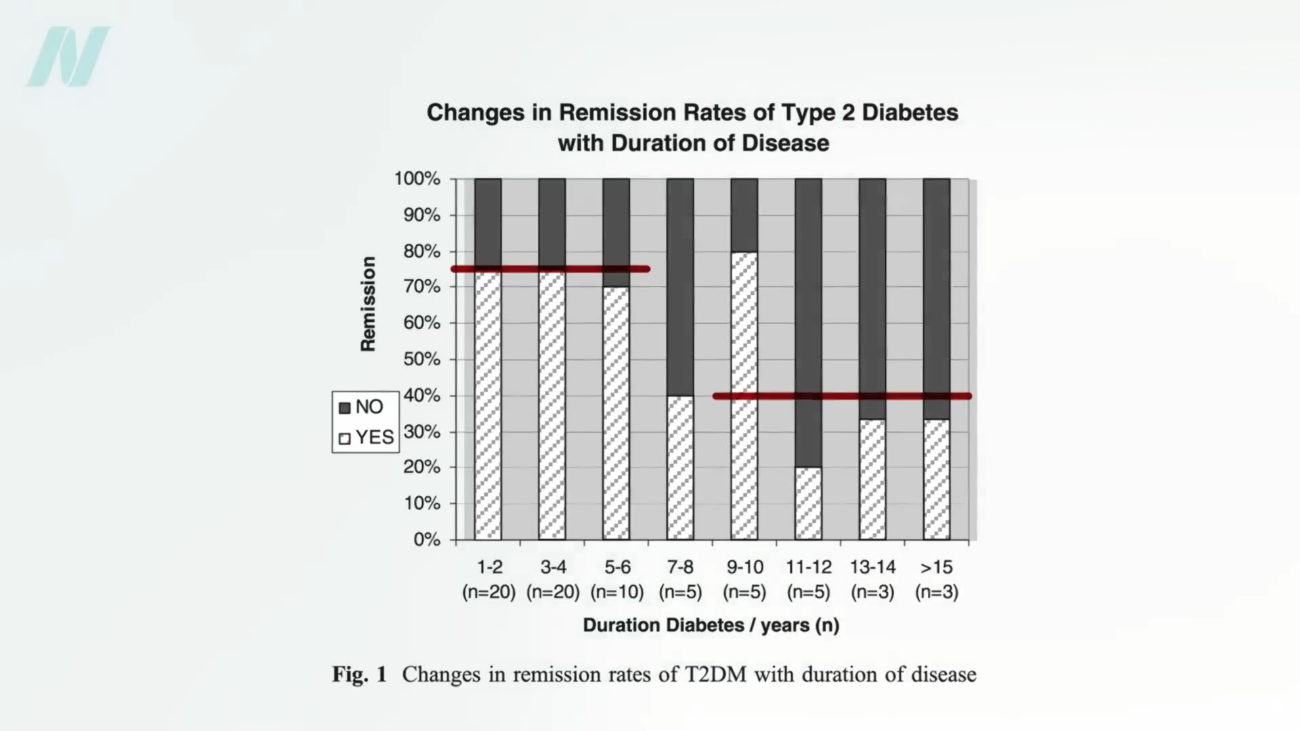
The implications of these findings extend to the broader understanding of diabetes remission and the role of weight loss. Research indicates that type 2 diabetes is indeed reversible, particularly in its earlier stages, through effective weight loss. Studies suggest that losing more than 30 pounds (13.6 kilograms) can lead to diabetes remission in nearly 90% of individuals who have had the disease for less than four years. However, for those who have lived with diabetes for eight years or more, the remission rate through diet alone may decrease to around 50%.
When comparing these figures to bariatric surgery, the distinction becomes even more pronounced. While bariatric surgery can lead to greater overall weight loss, the remission rates for diabetes appear to plateau. For patients who have had diabetes for up to six years, remission rates after bariatric surgery hover around 75%, and for those with longer-standing diabetes, this figure drops to approximately 40%. This suggests that while surgery facilitates substantial weight loss, the ability to reverse diabetes may be more closely tied to the duration of the disease and the underlying physiological changes that can be achieved through diet.
Beyond Blood Sugar: Systemic Inflammation and Diabetic Complications
The benefits of weight loss through diet alone may extend beyond glycemic control. Individuals who achieve weight loss through dietary interventions have demonstrated significant improvements in markers of systemic inflammation, such as tumor necrosis factor. In contrast, studies have shown that when a similar amount of weight is lost through gastric bypass, levels of systemic inflammation have, in some instances, worsened. This raises concerns about the broader systemic health impacts of different weight loss modalities.
Furthermore, the impact of bariatric surgery on long-term diabetic complications warrants careful consideration. While reversing diabetes through surgery can improve kidney function, evidence suggests it may not effectively prevent the occurrence or progression of diabetic vision loss. This observation might be linked to the fact that bariatric surgery primarily addresses the quantity of food consumed rather than the quality of the diet itself. This echoes findings from landmark studies, such as one published in The New England Journal of Medicine, which randomized thousands of individuals with diabetes to an intensive lifestyle program. After ten years, the study was halted early, as participants in the intensive lifestyle group did not show improved longevity or a reduced incidence of heart attacks. A potential explanation offered was that while participants consumed less food, they may have continued to consume the same types of heart-clogging dietary patterns in smaller portions.
Implications for Clinical Practice and Patient Guidance
The growing body of evidence suggesting that the profound metabolic benefits observed after bariatric surgery may be largely driven by the concurrent caloric restriction presents a critical juncture for clinical practice and patient guidance. It underscores the potent therapeutic power of diet and the potential for non-surgical interventions to achieve significant and lasting remission of type 2 diabetes.
This does not negate the role of bariatric surgery entirely, as it remains a valuable tool for individuals with severe obesity facing significant health challenges. However, it strongly advocates for a more comprehensive and individualized approach to treatment. Patients with type 2 diabetes and obesity should be thoroughly informed about the potential benefits and risks of both surgical and non-surgical weight loss strategies, with a clear understanding of the underlying mechanisms at play.
The emphasis on sustainable weight loss through dietary modification, rather than solely relying on anatomical alteration, aligns with a growing movement towards holistic health and preventative medicine. Further research is warranted to explore optimal dietary strategies for diabetes remission, long-term maintenance, and the prevention of diabetic complications. As the medical community continues to refine its understanding of metabolic diseases, the focus on evidence-based, patient-centered care, prioritizing the least invasive yet most effective interventions, will be paramount. The journey towards reversing type 2 diabetes may be less about rearranging the internal plumbing and more about recalibrating the fuel source.
A Doctor’s Perspective: Continuing the Conversation
This exploration into the efficacy of bariatric surgery in managing type 2 diabetes is part of an ongoing series aiming to provide a comprehensive overview of weight-loss interventions. Previous discussions have delved into "The Mortality Rate of Bariatric Weight-Loss Surgery" and "The Complications of Bariatric Weight-Loss Surgery," providing essential context for understanding the multifaceted nature of these procedures.
For individuals seeking guidance on achieving sustainable weight loss, resources such as the book How Not to Diet offer in-depth strategies focused on long-term success through nutritional science. The principle remains consistent: understanding the body’s intricate mechanisms and leveraging evidence-based approaches are key to navigating the complexities of weight management and metabolic health. The ultimate goal is to empower individuals with the knowledge and tools to make informed decisions that lead to improved health outcomes and a better quality of life, free from the burden of chronic disease.
